Chronic lymphocytic leukemia
What is chronic lymphocytic leukemia?
Chronic lymphocytic leukemia (CLL) is a neoplastic disease originating from B lymphocytes, characterized by clonal proliferation of tumor cells and accumulation of morphologically mature lymphocytes in the body. This leads to increased lymphocytes in peripheral blood and bone marrow, causing lymphadenopathy, hepatosplenomegaly, and impaired immune function. It is a type of leukemia.
Patients with CLL may experience not only physical suffering but also psychological distress. However, it is important not to lose hope in treatment. If a family member or friend has CLL, please provide them with emotional support and encourage them to actively pursue treatment.
Which department should I visit for chronic lymphocytic leukemia?
English name: Chronic lymphocytic leukemia, CLL.
Alternative name: Chronic lymphocytic leukemia.
Department: Hematology.
What causes chronic lymphocytic leukemia?
The exact cause is unknown, but several factors are closely associated with the disease:
- Monoclonal B-cell lymphocytosis (MBL): Multiple factors contribute to MBL formation, such as antigen stimulation, microenvironment changes, gene mutations, epigenetic modifications, and cytogenetic abnormalities. This results in B-cell clones with a CLL phenotype, which may rarely progress to CLL.
- Genetic factors: Individuals with a family history of CLL or other lymphoid malignancies have a threefold higher incidence rate among first-degree relatives compared to the general population. The incidence of immune system disorders is also significantly increased in relatives of CLL patients.
- Chromosomal abnormalities: The most common abnormalities include 13q deletion, 11q deletion, trisomy 12, and 17p deletion. Interphase fluorescence in situ hybridization (FISH) can detect chromosomal abnormalities in >80% of patients.
Who is most commonly affected by chronic lymphocytic leukemia?
CLL has a higher incidence in Western countries (particularly among Caucasians) but is less common in China, though the incidence is increasing yearly. It predominantly affects individuals over 50 years old, with incidence rising with age, and is more common in males than females.
What are the early and late symptoms of chronic lymphocytic leukemia?
The disease progresses slowly, often without noticeable symptoms. Many patients are diagnosed during routine check-ups or while seeking treatment for other conditions. Symptomatic patients may exhibit:
- Non-specific symptoms like fatigue and weakness.
- Anemia or thrombocytopenia.
- Lymphadenopathy (60–80% of patients), commonly in the neck, supraclavicular, and axillary regions, usually painless.
- Hepatosplenomegaly in about half of patients.
- Increased susceptibility to infections due to weakened immune function.
What are the diagnostic criteria for chronic lymphocytic leukemia?
CLL is suspected in adults with absolute lymphocytosis. Further evaluation includes: complete blood count with differential, peripheral blood flow cytometry to determine lymphocyte immunophenotype, and peripheral blood smear examination. Bone marrow examination is usually unnecessary unless cytopenia is unexplained.
CLL diagnosis requires meeting all three criteria:
- Peripheral blood B-lymphocyte count ≥5 × 109/L for ≥3 months.
- Peripheral blood smear showing predominantly small, mature lymphocytes.
- Flow cytometry confirming clonality of B lymphocytes via immunoglobulin light chain restriction (κ or λ).
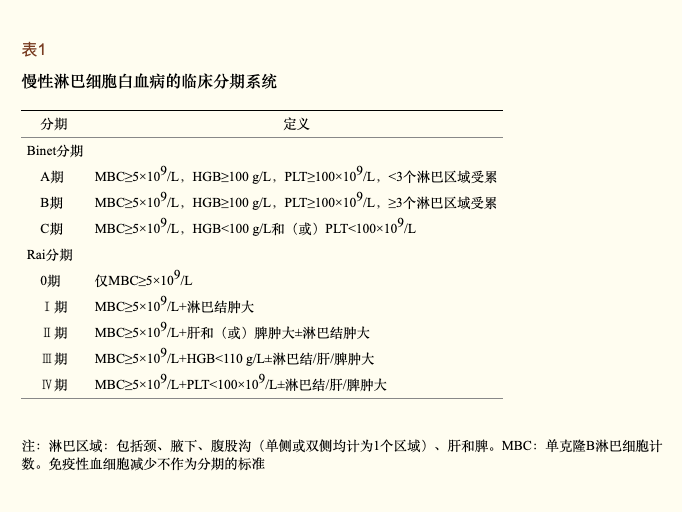
How is chronic lymphocytic leukemia staged?
Prognosis is commonly assessed using the Rai and Binet clinical staging systems (Table 1). Both rely on physical examination and basic lab tests, without requiring imaging like ultrasound, CT, or MRI.
How is chronic lymphocytic leukemia treated?
Treatment depends on clinical stage, symptoms, and disease activity. CLL has an indolent course, and early treatment does not improve survival. Patients in early stages (Rai 0–I or Binet A) require only regular monitoring.
If treatment is needed, options include:
- Chemoimmunotherapy: FC regimen (fludarabine + cyclophosphamide); FCR regimen (fludarabine + cyclophosphamide + rituximab).
- Radiotherapy: Whole-body or localized irradiation may improve symptoms but has short-lasting effects and often causes myelosuppression.
- Corticosteroids: Prednisone is commonly used.
- Bone marrow transplantation: Allogeneic or autologous hematopoietic stem cell transplantation.
- Targeted therapies: E.g., ibrutinib (BTKi), BCL-2 inhibitors.
- CAR-T cell therapy.
Is chronic lymphocytic leukemia curable? What is the prognosis?
A few patients may transform into prolymphocytic leukemia (PLL), which has poor treatment outcomes and shorter survival.
Richter transformation may occur, where CLL progresses into other lymphoid malignancies, often with rapid deterioration.
How can chronic lymphocytic leukemia be prevented? What precautions should be taken?
Since the cause is unknown, no specific prevention exists. General recommendations include:
- Maintain a healthy diet, exercise moderately, boost immunity, and avoid ionizing radiation.
- Middle-aged and elderly individuals should undergo regular check-ups for early detection and treatment.
- If relapse occurs after treatment, the regimen should be chosen based on the duration of remission after first-line therapy.